Prevalence of SARS-CoV-2 lineages of potential epidemiological concern at international level
Published: 04 August 2021
Two non-overlapping time intervals are compared to illustrate the circulation of VOCs in space. Table 1 incorporates data from July 14th (last update) to July 27th 2021, while Table 2 reports equivalent data for the interval considered in the previous update (from June 16th to July 13th 2021). Finally, the bar plots provide a graphical representation of the data.
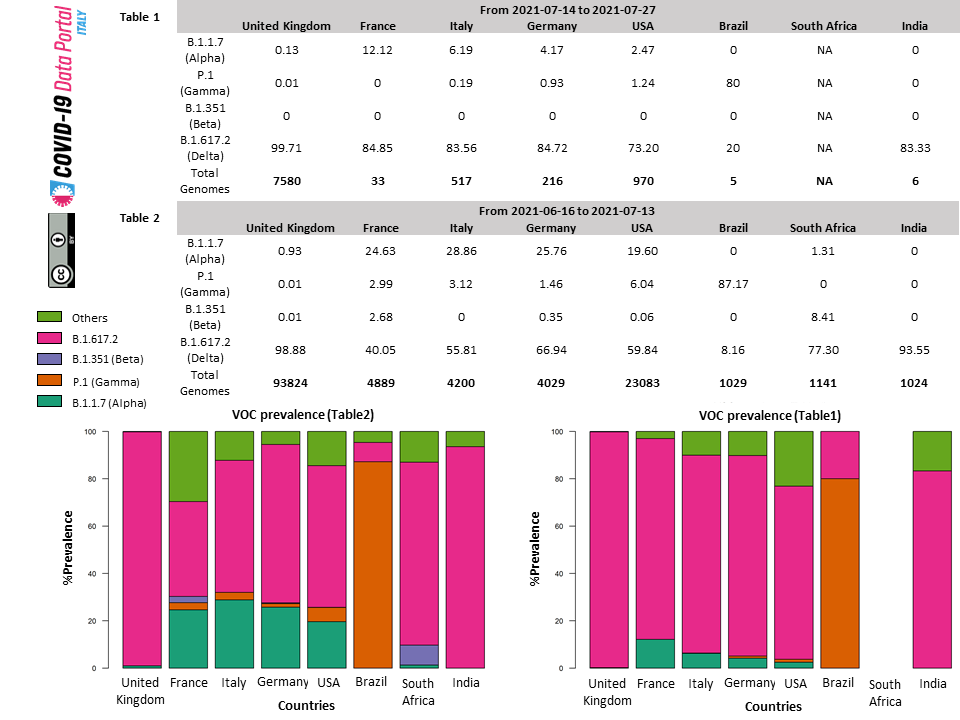
Table 1 reports the prevalence of the four VOCs in different countries (both European and extra-European) between July 14th and July 27th 2021.
Table 2 shows equivalent data but for the interval considered in the previous update (from June 16th to July 13th 2021). In both tables the last row indicates the total numbers of genomic sequences available at the time of analysis. The bar plots provide a graphical representation of the data reported in Table 1 and Table 2.
IMPORTANT: despite being as complete and up to date as possible, the analyses reported here can not provide a precise overview of the real epidemiological situation. In fact, available data are fragmented and do not possess the same level of completeness and accuracy for different geographic regions and countries. Increasing the number of viral genomes regularly sequenced and shared in public open access repositories, would be exential to improve the above-mentioned issue in the future.
Variants of potential epidemiological relevance
B.1.1.7 (Alpha variant)
B.1.1.7 was first detected in the South of the UK in mid-December 2020. This lineage has been shown to have higher transmissibility. Moreover, preliminary observations suggest also a greater severity of the disease, although further experimental tests and clinical investigations are required.
B.1.1.7, has been the most prevalent lineage of SARS-CoV-2 in Europe during the last winter and spring, however the prevalence of this lineage is decreasing steadily, as it is being replaced by the B.1.617.2 (Delta) variant in several European countries (see the previous updates/highlights from June 24th and July 17th).
As of July 27th 2021, B.1.1.7 presence was verified in 182 countries in the world.
Comparison between the values reported in Table 1 and Table 2, highlights a further decrease in the prevalence of B.1.1.7 in Italy, where its prevalence dropped from 28.86% to 6.19%. A similar pattern can be observed also in other European countries where the prevalence of the Alpha variant is significantly decreased (and in some cases almost halved) with a drop in prevalence, from 24.63% to 12.12% in France and a similar reduction from 25.76% to 4.17% in Germany. In the United Kingdom, the country where B.1.1.7 was first isolated, B.1.1.7 prevalence has decreased up to 0.13%. Importantly, for all the countries where a decrease in prevalence of B.1.1.7 is observed, a contemporary increase in the prevalence of the Delta variant (B.1.617.2) is recorded.
When extra-european countries are considered, a similar pattern of reduction in the prevalence of B.1.1.7 and contemporary increase of B.1617.2 can be observed in the United States (Alpha from 19.60% to 2.47% and Delta from 59.84% to 73.20%). A very marginal prevalence of the Alpha variant is reported in Brazil, whereas at the moment no new data are available to evaluate prevalence of B.1.1.7 or other variants in South Africa in the interval of time considered in this highlight. In India the prevalence of this variant is still close to 0.
P.1 (Gamma variant)
The P.1 lineage was first reported in Japan on January 19th 2021 where it was isolated in four travellers arriving from Brazil, and subsequently identified also in South Korea, again in travellers from the same country. Preliminary investigations in Manaus, Amazonas state, report an increase in the proportion of COVID-19 cases associated with P.1, from 52.2% (35/67) in December 2020 to 85.4% (41/48) in January 2021. The P.1 VOC is considered to have a greater transmissibility and propensity for reinfection, although available data are still limited. There is no evidence of increased severity of the disease.
As of July 27th 2021, P.1 was detected in 81 countries in the world.
The comparison between Table 1 and Table 2 shows how this lineage is still predominant in Brazil (where it was first identified) and its prevalence, even if slightly decreased, settled down around 80%.
Regarding other countries considered in this analysis, the overall prevalence of this variant remains generally low. At the time of the present update the prevalence of the Gamma variant is around 0.19% in Italy.
B.1.351 (Beta variant)
The B.1.351 lineage was first identified in South Africa in December 2020, where it was the most widespread viral type for a long time. Preliminary data indicate that this lineage may also be characterized by greater transmissibility, while it is currently unclear whether it is associated with more severe clinical manifestations.
As of July 27th 2021, B.1.351 presence was verified in 131 countries in the world.
As it can be clearly observed from data reported in Table 1 and Table 2, B.1.351 shows a limited prevalence outside of South Africa. However due to lack of data from South Africa, in the interval of time herein considered, no updates concerning the prevalence of the Beta variant in that country can be provided at this time.
B.1.617.2 (Delta variant)
B.1.617.2 was first identified in India during December 2020 and rapidly became the most prevalent lineage in the country, leading, as of April 2021, to a wide increase in daily hospitalization cases and deaths and, consequently, to a health system overload.
The Delta variant is considered to be 60% more infectious than the Alpha variant, additionally Delta is recognized less effectively by some neutralizing antibodies, and therefore can partially escape the immune response in people infected with other variants of the virus.
As of July 27th 2021, B.1.617.2 was recorded in at least 132 countries in the world.
It is evident from the data reported in Table 1 and Table 2 that B.1.617.2 is the most prevalent lineage in India (the country where this lineage was first isolated) and currently represents 83.33% of SARS-CoV-2 genomes reported from that country. In the last fifteen days a small increase in B.1.617.2 prevalence, from 98.88% to 99.71%, can be observed also in the United Kingdom. Notably all the countries herein considered, both European and extra-European, show a generalized and significant increase in the circulation of the Delta variant: from 40.05% to 84.85% in France, from 55.81% to 83.56% in Italy, from 66.94% to 84.72% in Germany, from 59.84% to 73.20% in the United States and from 8.16% to 20% in Brazil.
Sources: GISAID (genomic data), ECDC (Variants of Concern), WHO (epidemiological data)